
Medical Evacuation Concepts and Capabilities Division (MECCD)
Written by: Mr. George Hildebrandt, SFC Michael Bishop, SFC Billy Raines, and Mr. Lance Jones.
Army Aeromedical Evacuation has been the sole platform for intra-theater patient movement for the last twenty years of conflict. During that time we have seen changes across the fleet and community from the airframe, mission equipment, and medical equipment sets to the air ambulance provider’s skill set. Efforts continue to modernize the current capability, as well as development of the future MEDEVAC platform(s). As a result of several studies, lessons learned, and end user feedback; modernization efforts are focused on a redesigned patient care area that creates space, modularity, and environment to meet the needs of the unit, mission, commander, provider, and patient.
In 2015, Medical Evacuation Concepts and Capabilities Division (MECCD) worked with the United States Army Aeromedical Research Laboratory (USAARL) to conduct the Aeromedical Evacuation Enroute Critical Care Validation Study (i.e., Space Study).

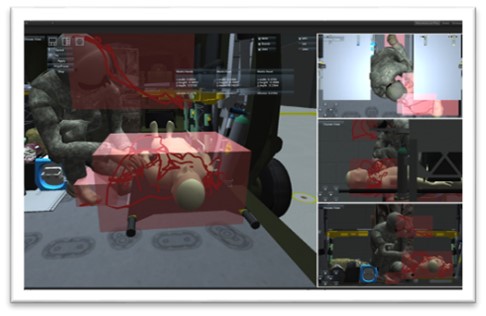
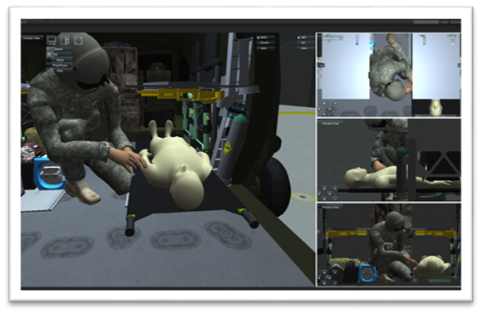
This study assessed the amount of vertical and horizontal space the Critical Care Flight Paramedic (CCFP) required to perform enroute care, which ultimately changed the minimum required vertical treatment space from 18 inches to 26 inches. In September 2019, another study was completed to assess the task saturation levels of the CCFP. The study identified the need for placing patient care items and supplies near the patient and the provider. These two studies provided the scientific rigor and data that informed the Capability and Material Developers when designing the next generation patient treatment areas.
MECCD and the Product Director for MEDEVAC (PD MEDEVAC) participated in information gathering events from deployed units. Units would describe the need to modify the cabin area by removing items to meet the required mission. For example, the current Patient Handling Systems would be removed, along with other systems such as the Oxygen Generation and Environmental Control Unit. This led to issues with reinstallation, including the inability to locate the required parts. The invaluable feedback received from these events provided the team with the lessons learned and tactics, techniques, and procedures which assisted with the overall design requirements.

Work on the next generation of Patient Handling Systems and the cabin area started following the MEDEVAC Mission Systems Capability Based Assessment in March 2015. From the beginning, it was recognized that the next generation system and redesigned cabin area must be modular to provide flexibility to the commander and provider based on the mission. Crews did not have hours to plan and prepare the aircraft for missions; they needed a system that could be adjusted to decrease weight, increase litter capacity, increase treatment space, increase attendant seats, or create a completely empty cabin to move supplies within minutes. It also had to have the ability to be reconfigured back to a different layout within minutes as well.

In between missions, the crew must be able to decontaminate and clean the interior cabin, while not having to remove all the equipment and systems to access even those places that had limited access. The floor must provide a barrier and assist in removing any biohazards that existed while also protecting the platform and integrating with the ballistic protection systems.
After years of gathering information, listening to the field, and assessing both current and future technologies, work is being done today to produce the first prototypes for the next generation Patient Handling Systems. The team of MECCD and PD MEDEVAC, along with key members from Telemedicine and Advanced Technology Research Center (TATRC), Naval Air Systems Command (NAVAIR), Medical Research & Development Command (MRDC), and the Future Vertical Lift Cross Functional Team (FVL-CFT), have worked diligently to design several system variants: one for the UH-60, one for the HH-60, and one for the FVL platform. While each platform has their own uniqueness; the floor, racks, and mounting systems will be virtually identical which will provide increased standardization. These same concepts are also being leveraged in the design of future ground evacuation platforms.
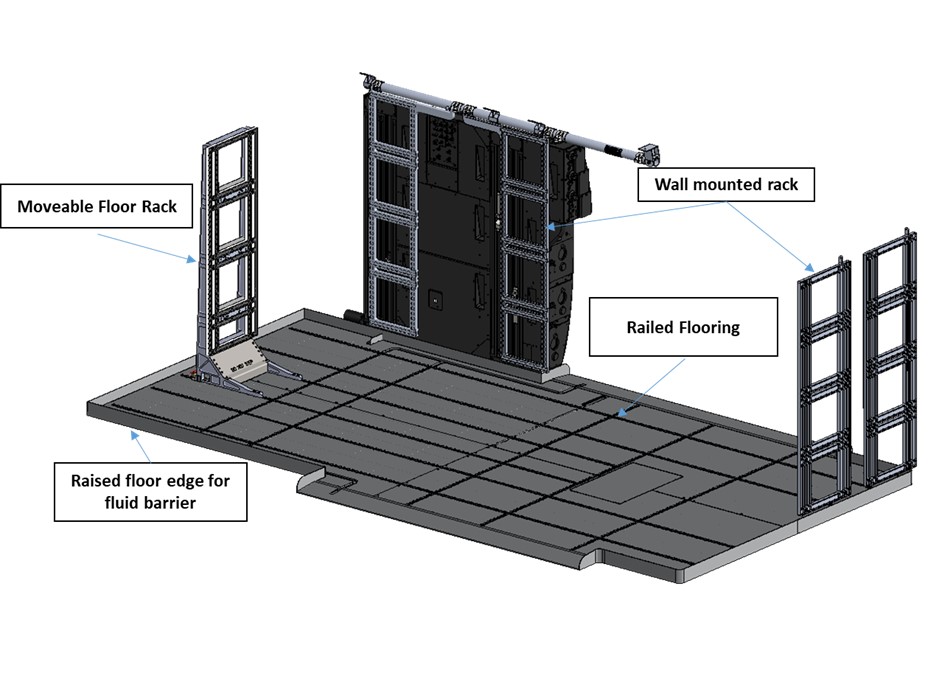
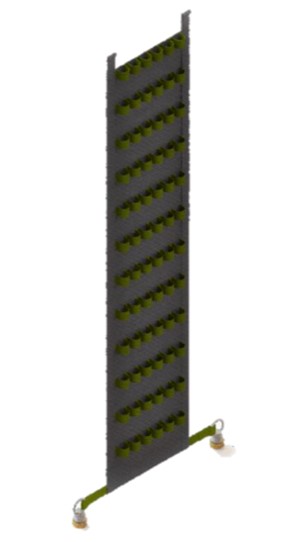
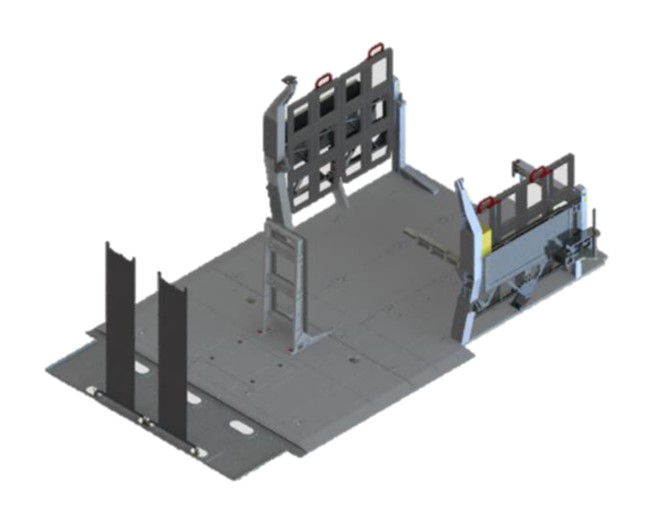
Each system starts out with the same design of a railed floor which enables the placement of floor mounted storage racks and creates channels directing fluid towards the cabin doors in order to assist with cleaning and removal of biohazards. The walls of the FVL cabin will have rail mounts attached to them, while the UH/HH-60s will have wall racks with rails that are mounted to the wall to provide securing points for medical equipment (e.g., monitor, suction, ventilator). Rail mounts allow the provider to place items wherever the rails are located. Items can be easily and quickly secured to a rail or removed and relocated to another location. Rails are placed in and around the litter stations of the Patient Handling System(s). Racks are designed with the same rail system which enables the crew to be able to move secured items throughout the cabin where they are readily available when needed. This provides units with the modularity required to configure the cabin based on mission requirements. One of the most significant changes to future platforms is there will not be integrated medical treatment systems (e.g., suction, oxygen); however, the current HH-60 will maintain the AMOGS/OBOGS system. All devices designed to provide direct care to patients will be carry-on items for all next generation Patient Handling Systems. This allows valuable flexibility when new technology emerges without having impact to the airframe. Litter pans can be easily removed or put back into place. Crew and passenger seats will be updated to integrate with the railed floor system. Other updates or changes include racks that allow different sized bottles or devices to be secured for oxygen along with lighting for patient care.

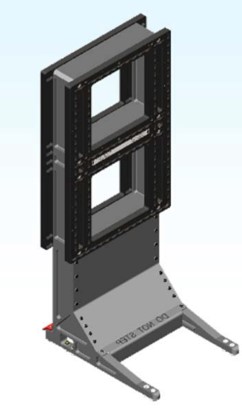
The wiring for 110v power outlets will not be integrated into the litter pan system and will thus be a standalone system. None of these racks or items require the Patient Handling System with litter pans to be installed in order to be available and can be placed in numerous locations throughout the cabin.
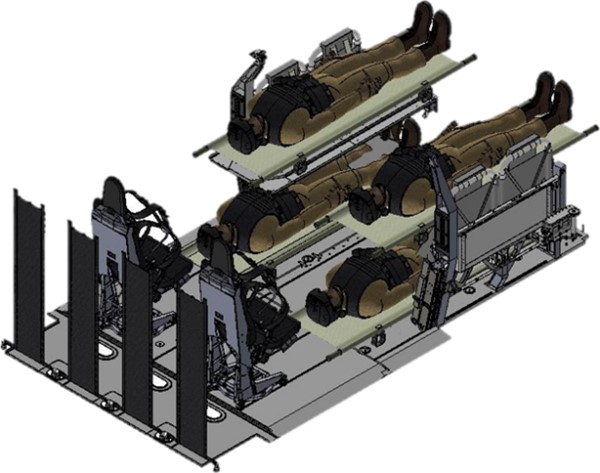
Design of the next MEDEVAC treatment area takes the future operating environment into consideration. Whether it be the severe cold in the Artic, the extreme heat of the Middle East, and/or disparate altitudes, the next system must enable units to operate in every location around the world. While the environment will have impact to aircraft performance, requiring adjustment to mission profile and weight limitations, we must also consider the amount of patients to be evacuated. In Large Scale Combat Operations (LSCO) the platform could be required to move six pre-surgical litter patients with the follow-on mission moving two post-surgical patients. The aforementioned considerations are what will drive the Aeromedical Evacuation Enterprise as we focus on these modernization efforts as, without the entire team and continuous feedback from the field, the ability to modernize the patient care area in order to provide the required enroute care for the injured warfighter would not be possible.